

Female Infertility
If you’re having trouble getting pregnant, your doctor will help you figure out why,
and work with you to find a treatment that can help.
What Causes Female Infertility?
There are a number of things that may be keeping you from getting pregnant:
Damage to your fallopian tubes. These structures carry eggs from your ovaries, which
produce eggs, to the uterus, where the baby develops. They can get damaged when scars form after pelvic infections, endometriosis, and
pelvic surgery. That can prevent sperm from reaching an egg. Hormonal problems. You may not be getting pregnant because your body isn’t going through the usual hormone changes that lead to the release of an egg from the ovary and the
thickening of the lining of the uterus. Cervical issues. Some women have a condition
that prevents sperm from passing through the cervical canal.
Uterine trouble. You may have polyps and fibroids that interfere with getting pregnant.
Uterine polyps and fibroids happen when too many cells grow in the endometrium, the lining
of the uterus. Other abnormalities of the uterus can also interfere,
“Unexplained” infertility. For about 20% of couples who have infertility pro
Tests for Infertility
Your doctor may order several tests, including a blood test to check hormone levels and an
endometrial biopsy to examine the lining of your uterus. Hysterosalpingography (HSG). This procedure involves ultrasound or X-rays of your reproductive
organs. A doctor injects either dye or saline and air into your cervix, which travel up through your
fallopian tubes. With this method, your doctor can check to see if the tubes are blocked.
Laparoscopy. Your doctor puts a laparoscope — a slender tube fitted with a tiny camera —
through a small cut near your belly button. This lets him view the outside of your uterus, ovaries,
and fallopian tubes to check for abnormal growths. The doctor can also see if your fallopian
tubes are blocked.
How Is Female Infertility Treated?
Laparoscopy. If you’ve been diagnosed with tubal or pelvic disease, one option is to get surgery to reconstruct your reproductive organs. Your doctor puts a laparoscope through a cut near your belly button to get rid of scar tissue, treat endometriosis, open blocked tubes, or remove ovarian cysts, which are fluid-filled sacs that can form in the ovaries. Hysteroscopy . In this procedure, your doctor places a hysteroscope into your uterus through your cervix. It’s used to remove polyps and fibroid tumors, divide scar tissue, and open up blocked tubes. Medication. If you have ovulation problems, you may be prescribed drugs such as clomiphene citrate (Clomid, Serophene), gonadotropins (such as Gonal-F, Follistim, Humegon and Pregnyl), or letrozole. Gonadotropins can trigger ovulation when Clomid or Serophene don’t work. These drugs also can also help you get pregnant by causing your ovaries to release multiple eggs. Normally, only one egg is released each month. Your doctor may suggest that you take gonadotropin if you have unexplained infertility or when other kinds of treatment haven’t helped you get pregnant. Metformin (Glucophage) is another type of medication that may help you ovulate normally if you have insulin resistance or PCOS (polycystic ovarian syndrome). Intrauterine insemination. For this procedure, after semen gets rinsed with a special solution, a doctor places it into your uterus when you’re ovulating. It’s sometimes done while you’re taking meds that help trigger the release of an egg. In vitro fertilization (IVF). In this technique, your doctor places into your uterus that were fertilized in a dish. You take gonadotropins that trigger the development of more than one egg. When the eggs are mature, your doctor collects them with a device called a vaginal ultrasound probe. Sperm are then collected, washed, and added to the eggs in the dish. Several days later, embryos — or fertilized eggs — get put back into your uterus with a device called an intrauterine insemination catheter. If you and your partner agree, extra embryos can be frozen and saved to use later. ICSI (intracytoplasmic sperm injection). A doctor injects sperm directly into the egg in a dish and then places it into your uterus. GIFT (gamete intrafallopian tube transfer) and ZIFT (zygote intrafallopian transfer). Like IVF, these procedures involve retrieving an egg, combining it with sperm in a lab, and then transferring it back to your body. In ZIFT, your doctor places the fertilized eggs — at this stage called zygotes — into your fallopian tubes within 24 hours. In GIFT, the sperm and eggs are mixed together before a doctor inserts them. Egg donation. This can help you if you have ovaries that don’t work right but you have a normal uterus. It involves removing eggs from the ovary of a donor who has taken fertility drugs. After in vitro fertilization, your doctor transfers the fertilized eggs into your uterus. Luteal Phase Defect If it’s hard for you to get pregnant or you get miscarriages, it’s possible that something called a luteal phase defect is playing a role. It’s a condition that disrupts your menstrual cycle, though there’s debate about whether it’s a direct cause of infertility and there is no way to really test to see if it is. See your doctor so he can figure out what’s going on and talk with you about your treatment options. What Is It? The luteal phase is one stage of your menstrual cycle. It occurs after ovulation (when your ovaries release an egg) and before your period starts. During this time, the lining of your uterus normally gets thicker to prepare for a possible pregnancy. If you have a luteal phase defect, that lining doesn’t grow properly each month. This can make it difficult to become or remain pregnant.
Causes of Luteal Phase Defect
The luteal phase is usually about 12 to14 days long. During this time, your ovaries make a hormone called progesterone. It tells the lining of your uterus to grow. When you get pregnant, your developing baby attaches to this thickened lining. If you don’t get pregnant, the lining eventually sheds, and you have a period. A luteal phase defect can happen to you if your ovaries don’t release enough progesterone, or if the lining of your uterus doesn’t respond to the hormone. The condition has been linked to many health
problems, including things like:
• Anorexia
• Endometriosis
• Extreme amounts of exercise
• Hyperprolactinemia (too much of a hormone that’s responsible for making breast milk)
• Obesity
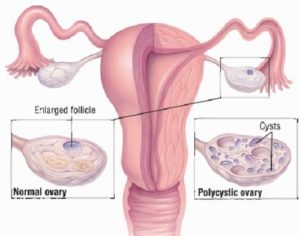
• Polycystic ovary syndrome
• Thyroid disorders
Many times, if you treat those conditions, you can correct your luteal phase defect.

Symptoms
When you have luteal phase defect, you may notice problems such as:
• More frequent periods
• Miscarriage
• Trouble getting pregnant
• Spotting between periods
Diagnosis
It may be hard for your doctor to pinpoint luteal phase defect as the source of your problems. There’s no single test that can diagnose it. He may suggest blood tests that can help figure out what’s happening, such as ones that check your levels of:
Follicle-stimulating hormone (FSH)
• Luteinizing hormone (LH)
• Progesterone
A pelvic ultrasound may also help your doctor measure the thickness of the lining of your uterus. In the past, your doctor may recommended a series of endometrial biopsies. He removes a small sample of the lining at a specific time of the month and examines it under a microscope to see if you were “in phase” or not. This is no longer done. Keep in mind that every woman can have luteal phase changes from time to time. The National Institutes of Health says that an endometrial biopsy can’t tell the difference between fertile and infertile women, so it doesn’t recommend it as a routine infertility test.
Treatment
What you do for this condition depends on your overall health and whether or not you’re trying to get pregnant. You’ll need treatment, of course, if you have any health problems that can lead to luteal phase defect. If you don’t want to get pregnant, you may not need any treatment. But if you’re trying to have a baby, your doctor may suggest medicines such as: Clomiphene citrate (Clomid). It triggers your ovaries to make more follicles, which release eggs. Human chorionic gonadotropin (hCG). It may help start ovulation and make more progesterone. Progesterone injections, pills, or suppositories. They may be used after ovulation to help the lining of your uterus grow. Talk to your doctor about all your treatment options. Studies have not proved that treating luteal phase defect improves the chances of a successful pregnancy in women who don’t use assisted reproduction techniques. Progesterone can help some women who get fertility treatments. But there’s no proof that taking it after you get pregnant will prevent a miscarriage.
Female Infertility: Causes, Treatment And Prevention
What causes female infertility?
The most common causes of female infertility include problems with ovulation, damage to fallopian tubes or uterus, or problems with the cervix. Age can contribute to infertility because as a woman ages, her fertility naturally tends to decrease.
Ovulation problems may be caused by one or more of the following:
- A hormone imbalance.
- A tumor or cyst.
- Eating disorders such as anorexia or bulimia.
- Alcohol or drug use.
- Thyroid gland problems.
- Excess weight.
- Stress.
- Intense exercise that causes a significant loss of body fat.
- Extremely brief menstrual cycles.
Damage to the fallopian tubes or uterus can be caused by one or more of the following:
- Pelvic inflammatory disease.
- A previous infection.
- Polyps in the uterus.
- Endometriosis or fibroids.
- Scar tissue or adhesions.
- Chronic medical illness.
- A previous ectopic (tubal) pregnancy.
- A birth defect.
- DES syndrome (The medication DES, given to women to prevent miscarriage or premature birth can result in fertility problems for their children.)
Abnormal cervical mucus can also cause infertility. Abnormal cervical mucus can prevent the sperm from reaching the egg or make it more difficult for the sperm to penetrate the egg.
How is female infertility diagnosed?
Potential female infertility is assessed as part of a thorough physical exam. The exam will include a medical history regarding potential factors that could contribute to infertility.